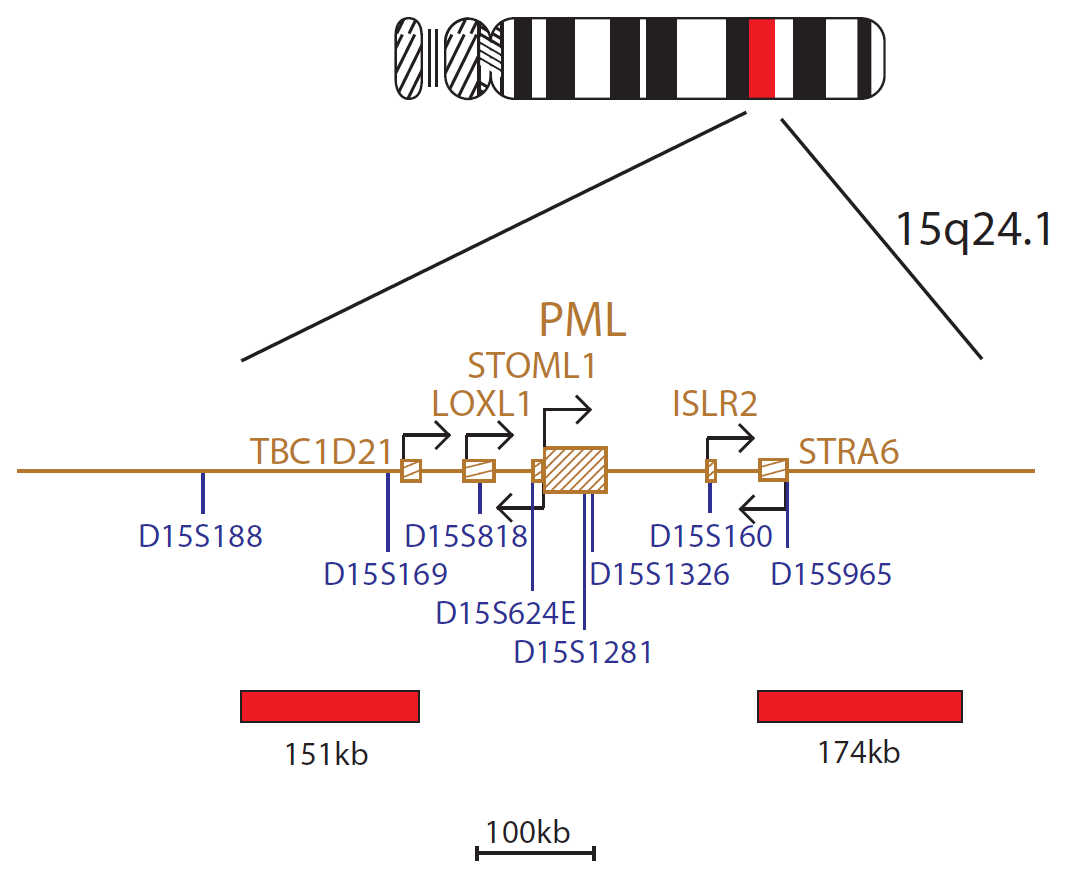
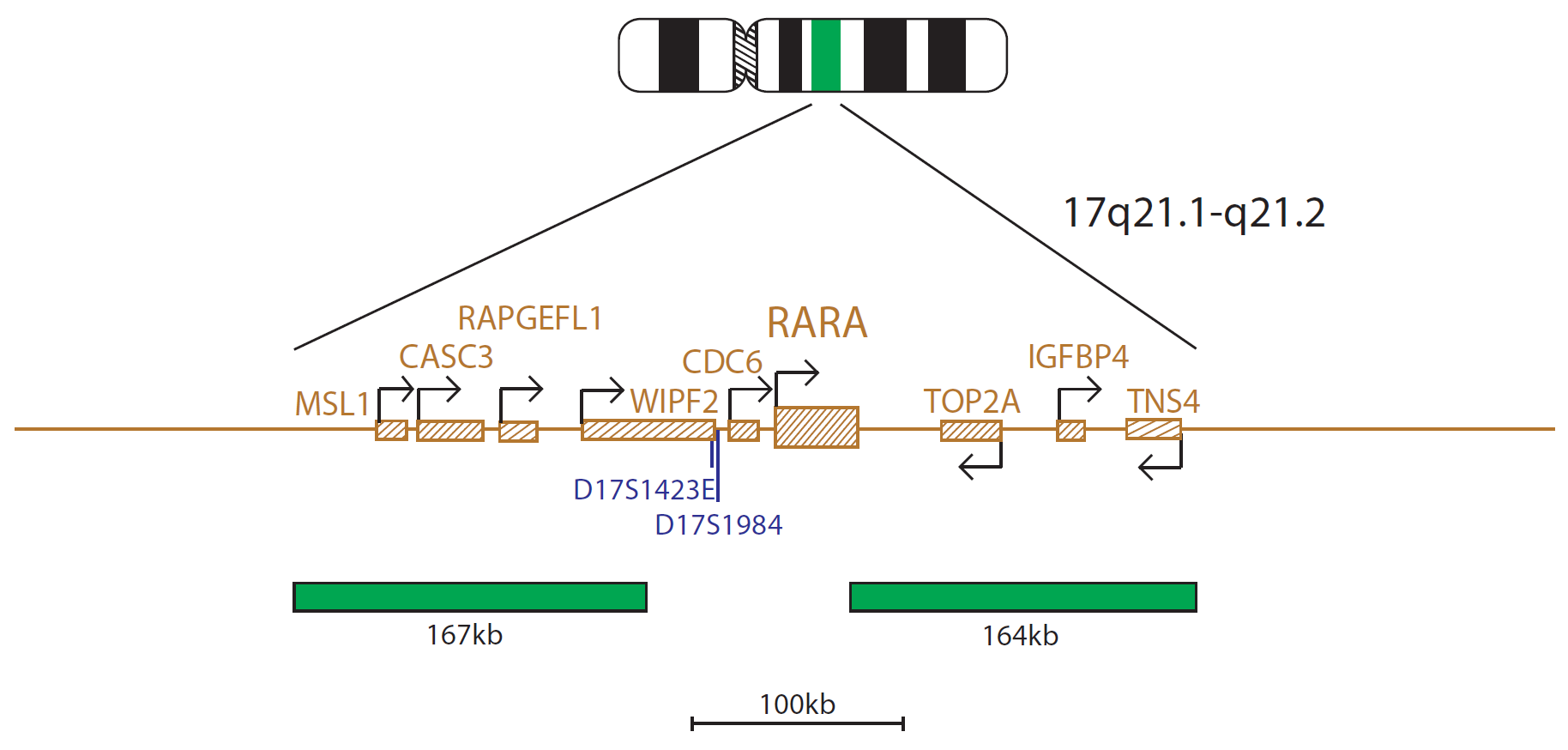
The PML probe mix, labelled in red, consists of a 151kb probe centromeric to the PML gene and a 174kb probe telomeric to the PML gene. The RARα probe mix, labelled in green, consists of a 167kb probe centromeric to the RARα (RARA) gene, including the CASC3 gene, and a 164kb probe, including the telomeric end of the RARα gene as well as the TOP2A and IGFBP4 genes.
The PML (promyelocytic leukemia) gene is located at 15q24.1 and the RARA (retinoic acid receptor alpha) gene is located at 17q21.2. The translocation t(15;17)(q24;q21) gives rise to the PML-RARA fusion gene and is the diagnostic hallmark of acute promyelocytic leukaemia (APL).
The PML-RARA fusion gene is created by the t(15;17)(q24;q21) translocation, found in more than 90% of cases of APL, a leukaemia that comprises 5-8% of cases of acute myeloid leukaemia (AML)1,2. In a subset of cases, variant RARA translocations can be observed. Known fusion partners include NPM1 at 5q35, NUMA1 at 11q13, ZBTB16 (PLZF) at 11q23, STAT5B at 17q21, PRKAR1A at 17q24, FIP1L1 at 4q12 and BCOR at Xp113,4,5.
PML and RARA have both been implicated in normal haematopoiesis. PML possesses growth suppressor and proapoptotic activity whereas RARA is a transcription factor that mediates the effect of retinoic acid at specific response elements6. PML-RARA fusion protein behaves as an altered retinoic acid receptor with an ability of transmitting oncogenic signaling7.
Immediate treatment of APL patients is critical, due to fatal coagulation disorders and life-threatening haemorrhage in diagnosis. Prior to the introduction of all-trans-retinoic-acid (ATRA) and arsenic trioxide (ATO) in APL treatment protocols, the disease had a poor prognosis; however, since the introduction of these therapies, the overall survival rate has improved dramatically, with nearly 90%5 of patients cured. Patients with variant RARA translocations show variable sensitivity to treatment, with some patients showing resistance to treatment protocols3,5. It is therefore important to differentiate between APL patients with PML-RARA fusion and those patients with variant RARA translocations.
Not only do CytoCell offer an extensive range of high-quality FISH probes, the customer support is also excellent — providing fast access to all the probes I need. The probes are highly consistent with bright signals allowing easy scoring of results.
Dr Eric Crawford
Senior Director, Genetics Associates Inc., USA

 Visit USA site
Visit USA site Visit Canada site
Visit Canada site