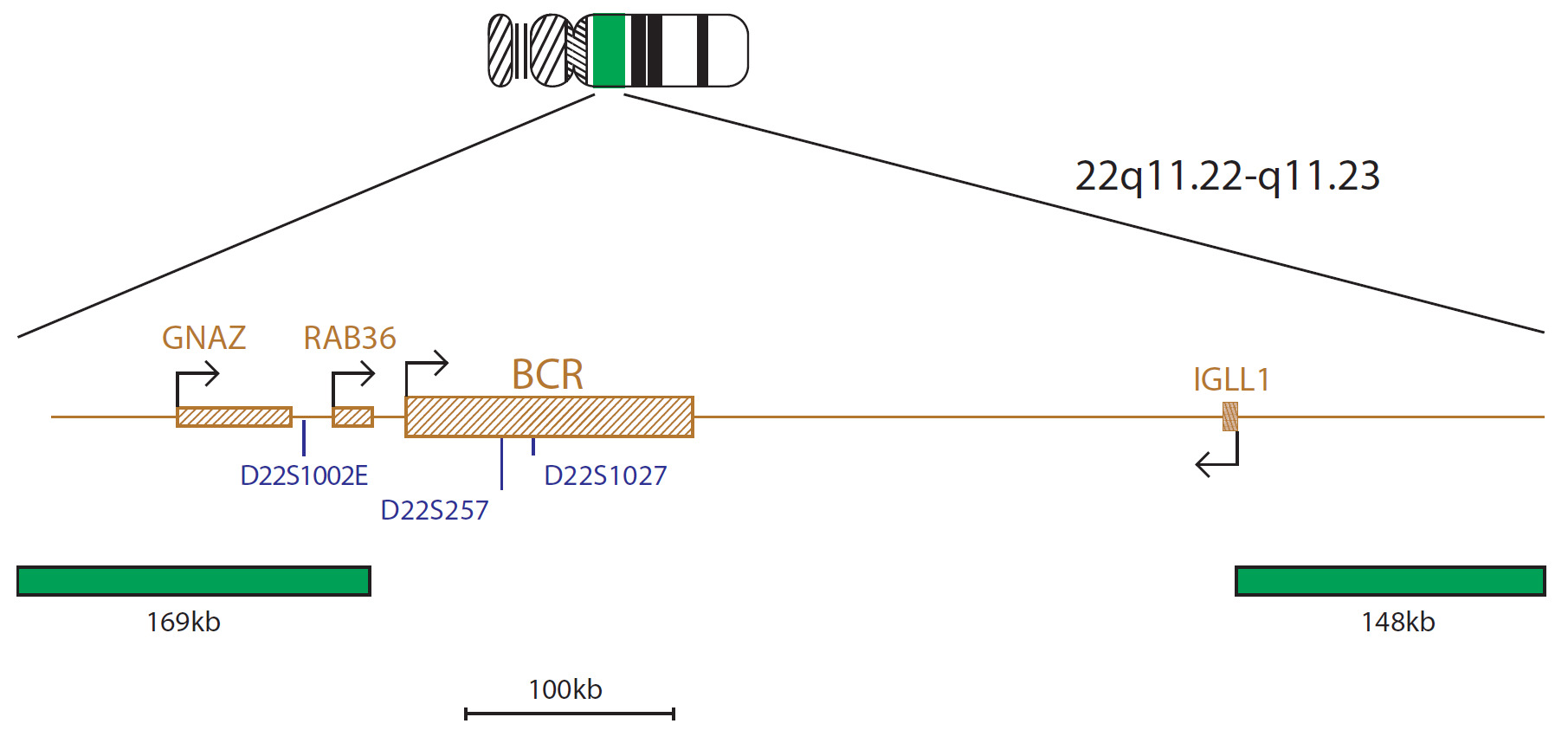
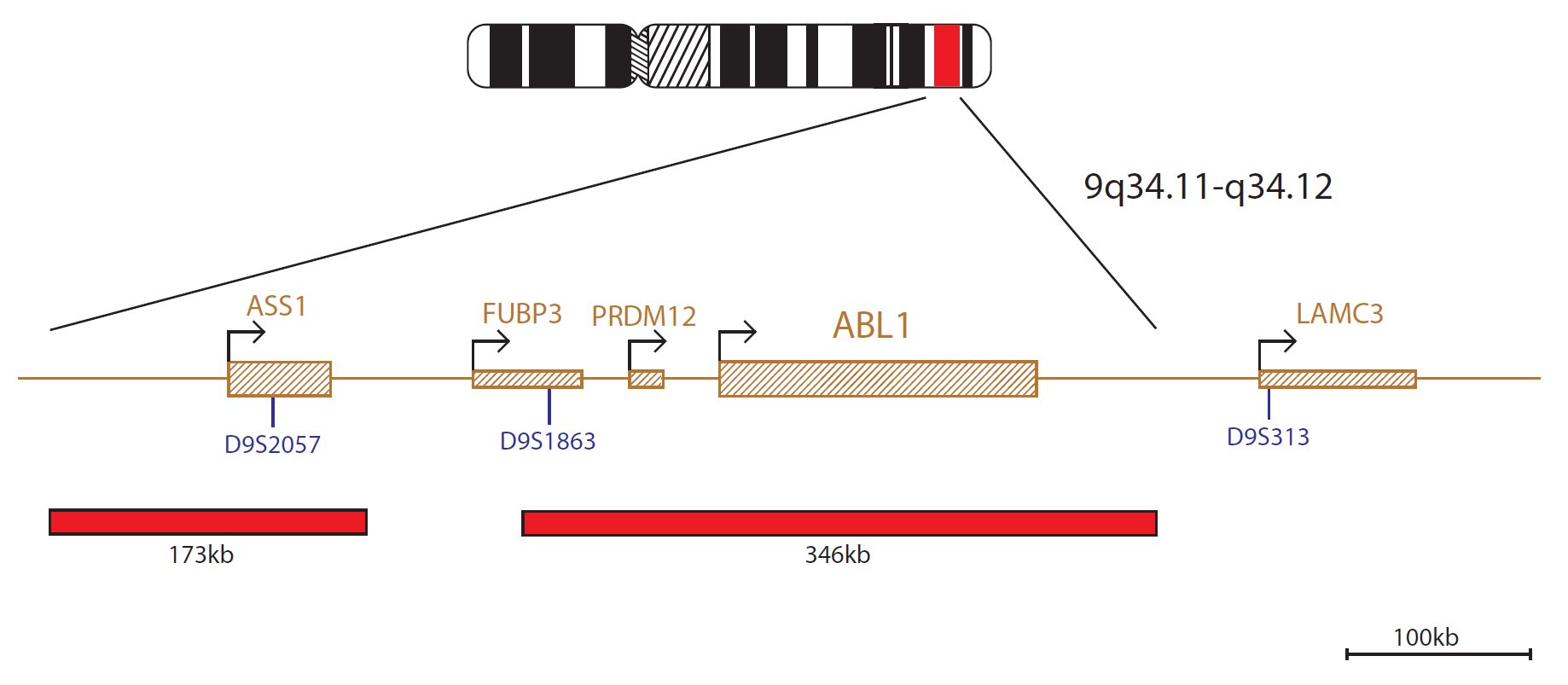
The BCR/ABL1 probe mix contains a 169kb green probe centromeric to the BCR gene and covers the genes GNAZ and RAB36. A second green probe covers a 148kb region that includes the telomeric end of the IGLL1 gene and the flanking region beyond. A red probe covers a 346kb region that includes the ABL1 gene. There is an additional red probe that covers a 173kb region and spans the whole ASS1 gene.
The BCR (BCR activator of RhoGEF and GTPase) gene is located at 22q11.23 and the ABL1 (ABL proto-oncogene 1, non-receptor tyrosine kinase) gene is located at 9q34.12. Translocation between these two genes gives rise to the BCR-ABL1 fusion gene, and produces a Philadelphia chromosome; the visible result of this translocation.
The presence of a BCR-ABL1 fusion has important diagnostic and prognostic implications in a number of haematological disorders.
The t(9;22)(q34.12;q11.23) translocation is the hallmark of chronic myeloid leukaemia (CML) and is found in around 90-95% of cases1. The remaining cases have a variant translocation, or have a cryptic rearrangement involving 9q34 and 22q11.23 that cannot be identified by routine cytogenetic analysis1.
The BCR-ABL1 fusion can also be found in 25% of adult acute lymphoblastic leukaemia (ALL) and in 2-4% of childhood ALL1. The presence of a BCR-ABL1 fusion has been shown to confer a poor prognosis in ALL in both adults and children1,2. The detection of the abnormality is therefore of high importance for risk stratification, which will influence treatment and management decisions2. In a small number of ALL cases, the translocation does not result in a cytogenetically visible Philadelphia chromosome. In these cases, FISH is essential for highlighting the fusion gene3.
This rearrangement is also seen in rare cases of acute myeloid leukaemia (AML). Philadelphia-positive AML is characterised by its resistance to conventional standard chemotherapy and poor prognosis4, so accurate and rapid identification of this chromosomal abnormality is vital.

Running our PETS protocol was taking upwards of 5 hours to complete based on the previous SOP. After the technical training visit from CytoCell, we were able to make some tweaks to reduce the protocol time down to just 1 hour and 15 minutes, with the same or better results.

Michelle Casey
Assistant Genetic Technologist, Leicestershire Genetics Centre, UK

 Visit USA site
Visit USA site Visit Canada site
Visit Canada site